CST works as a Complementary therapy... This means that if you suspect any serious condition or are worried about your health in any way, your first visit should be to your GP! The opinions expressed below are based on my clinical experience and the experience of my patients. CST is not a replacement for dental or orthodontic treatment.
CST provides a low impact, non-invasive, relatively inexpensive and non-surgical means to work with the structures of the face and jaw. So - what can it do and in what situations is it used? Some of the more common situations in which I have seen CST provide some help and relief include :
Braces, orthodontics and facial tightness
It's quite common for Cranial practitioners to find a correlation between various assymetric twists of the shoulder, neck, spine or hips - and a history of orthodontic braces. My personal feeling is that - the fact that somebody needed orthodontic treatment in the first place means that there was already a twist or tightness in their body which caused the teeth to move abnormally. However, what seems to happen in many cases of orthodontic treatment is that the face becomes rigid. This has some implications for structural (musculoskeletal) alignment and movement in the rest of the body.
As a practitioner, what I notice is that this rigidity of the face is far more common after braces have been worn, though it does occur in other circumstances - particularly when there is chronic emotional tension. I have also seen many times how patients report feeling their face softer and more comfortable when this tightness is released. And often there are other beneficial effects on the alignment and muscular tone around the neck, spine. Surprisingly, the knees are affected by the position of the tongue (see 2014 study the the Journal of Muscles, Ligaments & Tendons)!
Orthodontics can also sometimes be quite uncomfortable when applied. I have seen many cases where a small amount of CST not only helped the braces to feel more comfortable, but also assisted the progression of orthodontic correction. Some treatment prior to insertion and after the removal of orthodontics can also be useful.
Some dentists are now saying that Orthodontics may not be necessary given correct diet. Dr Mike Mew has a series of lectures on YouTube that show the main change in diet that has caused narrow faces (so that teeth need to be removed ) is that food for infants and children is too soft. See
his full length video. It's quite technical, but the upshot of it is that soft food does not exercise the face sufficiently and so it does not spread as it grows. Another very useful dental resource is a book published January 2018 by Dr Steven Lin
The Dental Diet. He points out many state of the art advances in nutritional research that show the "biome" (bacterial colony in the mouth) is as important for our health as the biome of the intestines. High fat diets protect the whole body, and insufficient fat of the correct type will result in ill health and dental decay. Again he emphasises chewing, since extended chewing foods high in fiber (rather than swallowing them quickly) releases short chain fatty acids that protect the teeth (and the entire digestive tract). Non-fatty acids (such as those released from refined sugars) dissolve the teeth.
Ascending and Descending
The jaw, shoulders and hips take part in a parallelogram-like arrangement that has a strong effect on the symmetry of the body and its movement. So, some people start with a jaw misalignment and end up with misaligned hips - because the hips respond to the jaw. This is termed a "Descending" TMJ issue, and (all other things being equal) is characterised by the pelvis tending to be OK provided that the person takes regular exercise such as running - which stabilises the lower half of the body. In many cases, Descending TMD results in pain experienced on waking (often in the hips) which goes after exercise. On the other hand, some people have a "Ascending" TMJ issue, in which case the TMJ is misaligned simply because the pelvis (or shoulders) is not straight. And of course, there are cases where both ends are slightly misaligned - often as a result of whiplash/RTAs. All of these respond well to CST treatment.
Clearly, Ascending and Descending issues require completely different types of treatment. Part of the differential diagnostic approach used in CST is to determine which effects are primary (and so treating them will have a permanent effect). If only the secondary adaptations are treated - which is usually the case where people just treat symptoms - it would be possioble to receive treatment for years with very little positive long term stability being achieved. With Symptomatic treatments, a beneficial effect might be felt for a few days or weeks, but then the problems just return again. If we can identify primary causes, far fewer treatments are necessary.
Why does the face/Jaw/TMJ affect the rest of the body so much?
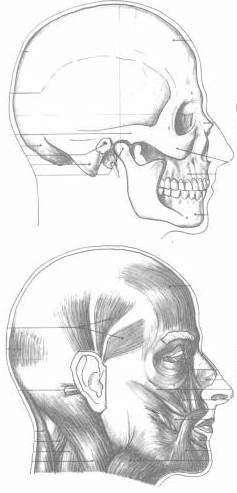
The face has to be very mobile so that emotional expression can occur (yes - the bones of the face also move when you smile or frown!), and so that the powerful forces of the jaw when eating can be accommodated. On the other hand, although the rest of the skull is somewhat mobile, it is far less mobile than the face. So there must be easy movement between the front of face and the more rigid skull/cranium. If this motion is compromised, there is a direct effect on important nerves and blood vessels; the lymphatic system protecting the central nervous system is not quite so effective, the balance of the head changes, and a dozen pairs of small muscles that connect to the face, tongue, jaw and base of the skull start to change the way that the neck and shoulders can move. Your body is a Holistic living organism, not a car - so small changes in one place can affect everything else!
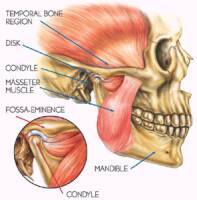
Upper and Lower jaws
When most people think of the Jaw, they actually think of the lower jaw - the jaw bone, or mandible. The TMJ (the joint for the lower jaw) sits just forward of the ear, and rests in a hollow of bone just a few millimetres from the middle and inner ear. Therefore the position of the lower jaw (and the muscular tension around it) affect the hearing and are one cause of hearing distortions and tinnitus. The lower jaw is unusual in the body in that it is a floating joint, and when we open our mouths very wide, the jaw joint semi-dislocates. Some animals (such as snakes) fully dislocate their jaws so that they can eat.
My clincial experience is that - for most cases - it is the position of the upper jaw (the face) that determines where the lower jaw sits! In fact, the relative position of the teeth (the occlusion) is sensitive to a few hundredths of a millimeter, and the teeth, being alive, move around in their sockets. The upper jaw (Maxilla) and its associated structures is rigid in parts, but most is as thin as paper and so is almost like the crumple zone of a car. Using gentle and non-manipulative Cranial techniques, it is possible to remobilise the face, which has substantial effects on the occlusion, on jaw stability and on the drainage of the face (including the Eustacian tubes and ears).
Further reading
 The Jaw and Face
The Jaw and Face